2023 Changes to Traditional MIPS
On November 1, 2022, the Centers for Medicare and Medicaid Services (CMS) issued the Final Rule for the 2023 Medicare Physician Fee Schedule (PFS) which includes several changes to the Quality Payment Program (QPP). The rule provides policy updates to the traditional Merit-based Incentive Payment System (MIPS) program, the new MIPS Values Pathway (MVPs) framework, Alternative Payment Models (APMs), and Accountable Care Organizations (ACOs).
CMS has adopted policy changes to traditional MIPS reporting in 2023:
The original framework for MIPS-eligible clinicians to collect and report data is known as Traditional MIPS. Clinician and group MIPS scores are determined by comparing their overall performance in the four MIPS categories (Quality, Improvement Activities, Promoting Interoperability, and Cost) to the CMS performance threshold score for a specific year.
For the 2023 performance year, the Final Rule set a minimum performance threshold of 75 MIPS points. The CMS continues to use the mean final score from the 2017 performance year to establish this threshold. Consequently, clinicians and groups must achieve 75 MIPS points in 2023 to avoid a negative payment adjustment in the 2025 payment year.
The 2022 MIPS Final Rule confirmed that there will no longer be an additional performance threshold for exceptional performance starting in 2023, with 2022 being the final year for earning an exceptional performance bonus.
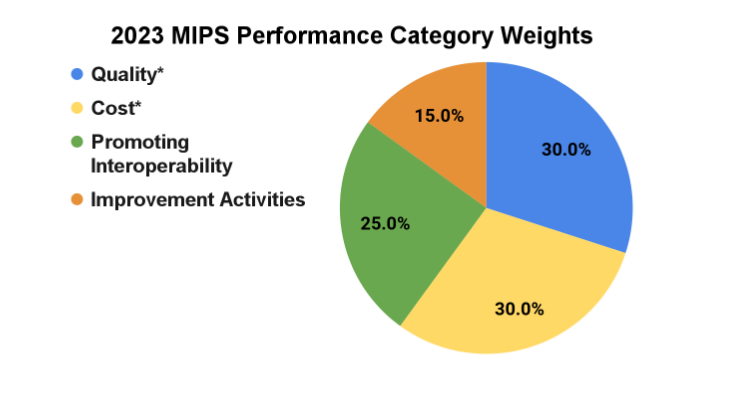
In 2023, CMS has not made any changes to the MIPS performance category weights and will continue to uphold the performance category redistribution policies for small practices (15 or fewer clinicians). The points from each category are combined to produce a final MIPS score.
MIPS Performance Category Weight Changes
By law, the Quality and Cost performance categories must be equally weighted at 30% beginning with the 2022 performance period. The weights for the Promoting Interoperability (25%) and Improvement Activities (15%) categories will remain the same as 2022.
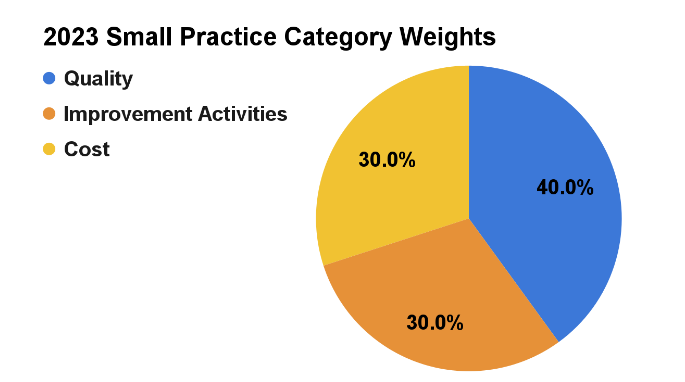
CMS will continue to automatically reweight the Promoting Interoperability performance category and more heavily weight the Improvement Activities performance category for small practices. When both Cost and Promoting Interoperability are reweighted, Quality and Improvement Activities will each be weighted at 50%.
Minimum Performance Threshold and Payment Adjustments
The payment adjustments for 2025 outlined in the table below reflect the removal of the additional adjustment for exceptional performance. MIPS scores at or below 18.75 points would earn the full -9 percent penalty.
| Final Score 2023 | Payment Adjustment 2025 |
|---|---|
| 75.01 - 100 points | Positive MIPS payment adjustment greater than 0% on a linear sliding scale |
| 75 points | 0% MIPS payment adjustment |
| 18.76 -74.99 points | Negative MIPS payment adjustment between -9% and 0% on a linear sliding scale |
| 0 - 18.75 points | Negative MIPS payment adjustment of -9% |
2023 Reweighting Policies
Large Practice Participants
The table below illustrates the 2023 performance category reweighting policies that CMS will apply to large practice participants (practice has 16 or more clinicians):
|
Reweighting Scenario |
Quality | Cost | Improvement Activities (IA) | Promoting Interoperability (PI) |
|---|---|---|---|---|
| No Reweighting Needed | ||||
| Scores for all 4 performance categories | 30% | 30% | 15% | 25% |
| Reweight 1 Performance Category | ||||
| No Cost | 55% | 0% | 15% | 30% |
| No PI | 55% | 30% | 15% | 0% |
| No Quality | 0% | 30% | 15% | 55% |
| No IA | 45% | 30% | 0% | 25% |
| Reweight 2 Performance Categories | ||||
| No Cost and no PI | 85% | 0% | 15% | 0% |
| No Cost and no Quality | 0% | 0% | 15% | 85% |
| No Cost and no IA | 70% | 0% | 0% | 30% |
| No PI and no Quality | 0% | 50% | 50% | 0% |
| No PI and no IA | 70% | 30% | 0% | 0% |
| No Quality and no IA | 0% | 30% | 0% | 70% |
Small Practice Participants
The table below illustrates the 2023 performance category reweighting policies that CMS will apply to small practice participants (practice has 15 or fewer clinicians):
| Reweighting Scenario | Quality | Cost | Improvement Activities (IA) | Promoting Interoperability (PI) |
|---|---|---|---|---|
| No Reweighting Needed | ||||
| Scores for all 4 performance categories | 30% | 30% | 15% | 25% |
| Reweight 1 Performance Category | ||||
| No Cost | 55% | 0% | 15% | 30% |
| No PI* | 40% | 30% | 30% | 0% |
| No Quality | 0% | 30% | 15% | 55% |
| No IA | 45% | 30% | 0% | 25% |
| Reweight 2 Performance Categories | ||||
| No Cost and no PI* | 50% | 0% | 50% | 0% |
| No Cost and no Quality | 0% | 0% | 15% | 85% |
| No Cost and no IA | 70% | 0% | 0% | 30% |
| No PI and no Quality | 0% | 50% | 50% | 0% |
| No PI and no IA | 70% | 30% | 0% | 0% |
| No Quality and no IA | 0% | 30% | 0% | 70% |
*The finalized redistribution policy specifically for MIPS eligible clinicians in small practices.
Quality Category Updates
CMS is maintaining the current data completeness requirements for the 2023 performance year, so clinicians will report at least 70% of eligible encounters for the quality measures they report, regardless of insurance type. However, this threshold increases to 75% for the 2024 and 2025 performance years.
There are a number of quality measure changes, including expansion of the definition of “high priority measure” to include health equity-related quality measures. CMS finalized a total of 198 quality measures for the 2023 performance period which reflect:
- Substantive changes to 76 existing quality measures;
- The addition of 9 new quality measures (which includes one new administrative claims measure);
- Removal of 11 quality measures; and
- Addition/removal of quality measures from multiple specialty sets.
Measures that have been added to or removed from the 2023 Quality measure inventory, along with their collection types, are outlined in the tables below.
| New Quality Measures | Collection Type |
|---|---|
| #485 Psoriasis – Improvement in Patient-Reported Itch Severity | MIPS Clinical Quality Measure (CQM) |
| #486 Dermatitis – Improvement in Patient-Reported Itch Severity | MIPS CQM |
| #487 Screening for Social Drivers of Health | MIPS CQM |
| #488 Kidney Health Evaluation | Electronic CQM (eCQM) and MIPS CQM |
| #489 Adult Kidney Disease: Angiotensin Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy | MIPS CQM |
| #490 Appropriate Intervention of Immune-Related Diarrhea and/or Colitis in Patients Treated with Immune Checkpoint Inhibitors | MIPS CQM |
| #491 Mismatch Repair (MMR) or Microsatellite Instability (MSI) Biomarker Testing Status in Colorectal Carcinoma, Endometrial, Gastroesophageal, or Small Bowel Carcinoma | MIPS CQM |
| #492 Risk-Standardized Acute Cardiovascular-Related Hospital Admission Rates for Patients with Heart Failure under the Merit-based Incentive Payment System | Administrative Claims* |
| #493 Adult Immunization Status | MIPS CQM |
*CMS will use performance period benchmarks exclusively for scoring administrative claims measures.
| Retired Quality Measures | Collection Type |
|---|---|
| #76 Prevention of Central Venous Catheter (CVC) - Related Bloodstream Infections | Medicare Part B Claims, MIPS CQM |
| #119 Diabetes: Medical Attention for Nephropathy | eCQM, MIPS CQMs |
| #258 Rate of Open Repair of Small or Moderate Non-Ruptured Infrarenal Abdominal Aortic Aneurysms (AAA) without Major Complications (Discharged to Home by Post-Operative Day #7) | MIPS CQM |
| #265 Biopsy Follow-Up | MIPS CQM |
| #323 Cardiac Stress Imaging Not Meeting Appropriate Use Criteria: Routine Testing After Percutaneous Coronary Intervention (PCI) | MIPS CQM |
| #375 Functional Status Assessment for Total Knee Replacement | eCQM |
| #425 Photodocumentation of Cecal Intubation | MIPS CQM |
| #455 Percentage of Patients Who Died from Cancer Admitted to the Intensive Care Unit (ICU) in the Last 30 Days of Life (lower score – better) | MIPS CQM |
| #460 Back Pain After Lumbar Fusion | MIPS CQM |
| #469 Functional Status After Lumbar Fusion | MIPS CQM |
| #473 Leg Pain After Lumbar Fusion | MIPS CQM |
| Quality Measures Removed from Traditional MIPS* | Collection Type |
|---|---|
| #110: Preventive Care and Screening: Influenza Immunization | Medicare Part B Claims, eCQM, MIPS CQM |
| #111: Pneumococcal Vaccination Status for Older Adults | Medicare Part B Claims, eCQM, MIPS CQM |
*These measures will still be available for MVP reporting. Measure #110 will also be retained for MSSP ACO reporting through the APP. When reporting under traditional MIPS, a new Adult Immunization Status measure will include influenza and pneumococcal vaccination, as well as Td/Tdap and Zoster vaccination.
Previously Finalized Quality Updates for 2023:
In the 2022 MIPS Final Rule several policy changes were adopted that go into effect beginning with the 2023 performance period:
- Measures with a benchmark - The 3-point floor is removed for measures that can be scored against a benchmark. These measures will receive 1-10 points. (This does not apply to new measures in the first 2 performance periods available for reporting.)
- Measures without a benchmark - The 3-point floor is removed for measures without a benchmark (except small practices). These measures will receive 0 points (small practices will continue to earn 3 points). (This does not apply to new measures in the first 2 performance periods available for reporting or to administrative claims measures.)
- Measures that don’t meet case minimum requirements (20 cases) - The 3-point floor is removed (except small practices). These measures will earn 0 points (small practices will continue to earn 3 points). (This does not apply to new measures in the first 2 performance periods available for reporting or to administrative claims measures. Measures calculated from administrative claims are excluded from scoring if the case minimum is not met.)
- New Measures - New measures in their 1st year in the program are subject to a 7-point scoring floor provided data completeness requirements are met. New measures in their 2nd year in the program are subject to a 5-point scoring floor provided data completeness requirements are met.
Cost Category Updates
A maximum cost improvement score of one percentage point out of 100 percentage points is established for the Cost performance category. It will be retroactively applied to start with the current 2022 performance period.
Improvement Activities Category Updates
There are no major changes to the MIPS Improvement Activities (IA) category other than updates to the IA inventory. CMS is adding four new activities, modifying five current activities, and removing five existing improvement activities from the IA inventory as outlined in the following table.
| New Improvement Activities | Retired Improvement Activities |
|---|---|
| IA_AHE_10 Adopt Certified Health Information Technology for Security Tags for Electronic Health Record Data (Medium) | IA_BE_7 Participation in a QCDR, that promotes use of patient engagement tools |
| IA_AHE_11 Create and Implement a Plan to Improve Care for Lesbian, Gay, Bisexual, Transgender, and Queer Patients (High) | IA_BE_8 Participation in a QCDR, that promotes collaborative learning network opportunities that are interactive |
| IA_EPA_6 Create and Implement a Language Access Plan (High) | IA_PM_7 Use of QCDR for feedback reports that incorporate population health |
| IA_ERP_6 COVID-19 Vaccine Achievement for Practice Staff (Medium) | IA_PSPA_6 Consultation of the Prescription Drug Monitoring program |
| IA_PSPA_20 Leadership engagement in regular guidance and demonstrated commitment for implementing practice improvement changes | |
| IA_PSPA_30 PCI Bleeding Campaign |
Promoting Interoperability Category Updates
CMS is making several changes to the Promoting Interoperability (PI) category. The updates include:
- Requiring and modifying the Electronic Prescribing Objective’s Query of Prescription Drug Monitoring Program (PDMP) measure.
- Expanding the Query of PDMP measure to include not only Schedule II opioids, but also Schedule III, and IV drugs.
- Adding a new Health Information Exchange (HIE) Objective option, the Enabling Exchange under the Trusted Exchange Framework and Common Agreement (TEFCA) measure (requiring a yes/no response), as an optional alternative to fulfill the objective.
- Consolidating the current options from three to two levels of active engagement for the Public Health and Clinical Data Exchange Objective and require the reporting of active engagement for the measures under the objective.
- Continuing to reweight the PI category for certain types of non-physician practitioner MIPS eligible clinicians.
CMS is discontinuing automatic reweighting for the following clinician types beginning with the 2023 performance period:
- Nurse practitioners
- Physician assistants
- Certified registered nurse anesthetists
- Clinical nurse specialist
The agency will continue automatic reweighting for the following in the 2023 performance period:
- Clinical social workers
- Physical therapists
- Occupational therapists
- Qualified speech-language pathologists
- Qualified audiologists
- Clinical psychologists, and
- Registered dieticians or nutrition professionals
When participating in MIPS at the APM Entity level (reporting the APP, traditional MIPS, or an MVP), CMS will allow APM Entities to report PI data at the APM Entity level. APM Entities will still have the option to report this performance category at the individual and group levels.
CMS is also updating PI scoring for each of the PI measures as follows:
| PI Objective | Measure | Maximum Points |
|---|---|---|
| Electronic Prescribing |
e-Prescribing | 10 points |
| Query of PDMP | 10 points | |
| Health Information Exchange |
Support Electronic Referral Loops by Sending Health Information | 15 points |
| Support Electronic Referral Loops by Receiving and Reconciling Health Information | 15 points | |
| OR | ||
| Health Information Exchange Bi-Directional Exchange* | 30 points | |
| OR | ||
| Participation in TEFCA | 30 points | |
| Provider to Patient Exchange | Provide Patients Electronic Access to Their Health Information | 25 points |
| Public Health and Clinical Data Exchange | Report the following 2 measures:
|
25 points |
| Report one of the following measures:
|
5 points (bonus) | |
Complex Patient Bonus
CMS finalized that a facility-based MIPS eligible clinician would be eligible to receive the complex patient bonus, even if they don’t submit data for at least one MIPS performance category.
MIPS Value Pathways (MVPs)
As previously finalized in the 2022 MIPS final rule, CMS will make MVPs available for reporting beginning with the 2023 performance year:
- 2023, 2024, and 2025 performance years - Individual clinicians, single specialty groups, multispecialty groups, subgroups, and APM Entities can report MVPs.
- 2026 performance year and for future years - Individual clinicians, single specialty groups, subgroups, and APM Entities can report MVPs. Multispecialty groups will be required to form subgroups to report MVPs.
CMS continues to focus on the development of MVPs and subgroup reporting and has finalized a total of 12 MVPs for the 2023 performance year.
Subgroup Registration
Clinicians who choose to participate in a subgroup to report an MVP must register as a subgroup between April 1 and November 30 of the performance year. In addition to the required MVP registration information*, the subgroup registration must include:
- A list of Taxpayer Identification Numbers (TINs)/National Provider Identifiers (NPIs) in the subgroup;
- A plain language name for the subgroup (which will be used for public reporting);
- A description of the composition of the subgroup, which may be selected from a list or described in a narrative.
Clinicians (identified by NPI) may register for one subgroup per TIN.
Subgroup Eligibility
CMS will use the first segment of the MIPS determination period to determine the eligibility of clinicians intending to participate and register as a subgroup. As previously finalized, each subgroup must include at least one MIPS eligible clinician.
Subgroup Scoring
CMS will calculate and score administrative claims measures at the TIN level, not at the subgroup level:
- Foundational Layer (MVP Agnostic) - For each selected population health measure in an MVP, subgroups would be assigned the affiliated group’s score, if available. In instances where a group score is not available, each such measure would be excluded from the subgroup’s final score.
- Quality Performance Category - For each selected outcomes-based administrative claims measure in an MVP, subgroups would be assigned the affiliated group’s score, if available. In instances where a group score is not available, each such measure would be assigned a zero score.
- Cost Performance Category - Subgroups would be assigned the affiliated group’s cost score, if available for the cost performance category in an MVP. In instances where a group score is not available, each such measure would be excluded from the subgroup’s final score.
Subgroup Final Score
CMS will not assign a score for a subgroup that registers but does not submit data as a subgroup.
Advanced APMs
CMS finalized the following policies to encourage participation in Alternative Payment Models (APMs):
- Makes permanent the 8% minimum on the Generally Applicable Nominal Risk standard for Advanced APMs.
- Applies the 50 clinician limit to the APM Entity participating in the Medical Home Model. CMS will identify the clinicians in the APM Entity by using the TIN/NPIs on the participation list of the APM Entity on each of the three QP determination dates (March 31, June 30, and August 31). This policy would become effective in performance year 2023.
Medicare Shared Savings Program (MSSP)
CMS finalized the following provisions that impact MSSP Accountable Care Organizations (ACOs):
- Changes the current “Pathways to Success” glide path to give ACOs more time before advancing to the highest levels of risk.
- Provides advance shared savings payments (“advance investment payments”) to low-revenue ACOs inexperienced with risk that serve underserved populations, including an upfront fixed payment and quarterly payments adjusted for beneficiaries’ social risk.
- Reinstates a sliding scale approach for determining shared savings for ACOs, regardless of how they report quality data.
- Establishes a health equity bonus to reward ACOs that report all-payer eCQMs/MIPS CQMs and serve a high proportion of underserved beneficiaries. The adjustment would add up to 10 bonus points to the ACO’s MIPS quality performance category score.
- Extends the incentive for reporting eCQMs/MIPS CQMs through performance year 2024 to align with the sunsetting of the CMS Web Interface reporting option.
- Changes certain aspects of its benchmarking methodologies aimed at improving participation among providers who treat a high percentage of beneficiaries with substantial clinical risk factors and dually eligible beneficiaries.